
TOLAC and VBAC: Conclusive Guidelines, Benefits And Risks 2024
As a woman and a mother, birth choices are deeply personal aspects of women’s health. As you begin the journey to motherhood, it will fill you with a variety of emotions, and at the end of the day, all you want to do is what is best for you and your baby.
However, during childbirth unexpected changes happen, and even though you didn’t plan for a cesarean delivery it may occur due to several reasons. Some moms feel they missed out on a unique experience and have hopes that if they become pregnant again, they’ll be able to have a trial of labor after cesarean (TOLAC). If that’s successful, then they will have gone on to have a VBAC or vaginal birth after cesarean.
It’s not a given that a woman who’s had a C-section will be able to give birth naturally the next time around, and in fact, there are several potential obstacles to that happening.
As a saying before “Once a cesarean, always a cesarean.” From 1916, when these words were spoken to the New York Association of Obstetricians & Gynecologists, through the ensuing 50-60 years, this statement reflected most US obstetricians’ management of patients with a prior cesarean delivery.
Between 1970 and 2016, the Cesarean-section (C-section) rate in the United States increased from 5% to 31.9%. The belief in “once a C-section, always a C-section” is one of the reasons that the C-section rate has increased. However, in 2010, the National Institutes of Health recognized that trying vaginal birth after C-section was a reasonable option for many women with a previous C-section.

Which created several settings of discussions and debates in the field of TOLAC (trial of labor after cesarean) and VBAC (vaginal birth after cesarean). In this article, we are going to give you conclusive guidelines, risks, and benefits of trial of labor after cesarean and vaginal birth after cesarean. This will provide information to women and caregivers who would like to try vaginal delivery after cesarean. Because without C-section incision pain, patients can also take care of their little ones more comfortably.
However, this is still a case-to-case basis, as there will be emergency C-sections when uterine rupture happens that can put the mother and the baby at risk. An emergent C-section is required at this time. So better to keep on reading to learn more!
TOLAC Overview
What is TOLAC?
Trial of labor after cesarean delivery (TOLAC) refers to a planned attempt to deliver vaginally by a woman who has had a previous cesarean delivery, regardless of the outcome. This method provides women who desire a vaginal delivery the possibility of achieving that goal—a vaginal birth after cesarean delivery (VBAC).
Risks of TOLAC:
- Infection
- Surgical injury
- Blood transfusion
- Hysterectomy
- Uterine rupture-results in the most significant increase in the likelihood of additional maternal and neonatal morbidity.
- Most maternal complications related to TOLAC occur when a repeat cesarean delivery becomes necessary. For example, a patient is laboring and attempting to have a VBAC, but a cesarean delivery is needed.VBAC is associated with fewer complications than elective repeat cesarean delivery, whereas a failed TOLAC is associated with more complications.
- The decision to undergo TOLAC or repeat cesarean section should be documented and included in the medical record. Clinicians should document a review of the counseling session, including the potential risks and benefits of both TOLAC and elective repeat cesarean section, as well as a management plan.

TOLAC Success Rate
The success rate is influenced by various factors including prior vaginal delivery, the reason for the prior cesarean delivery, and the circumstances surrounding the previous cesarean birth.
Candidates for TOLAC
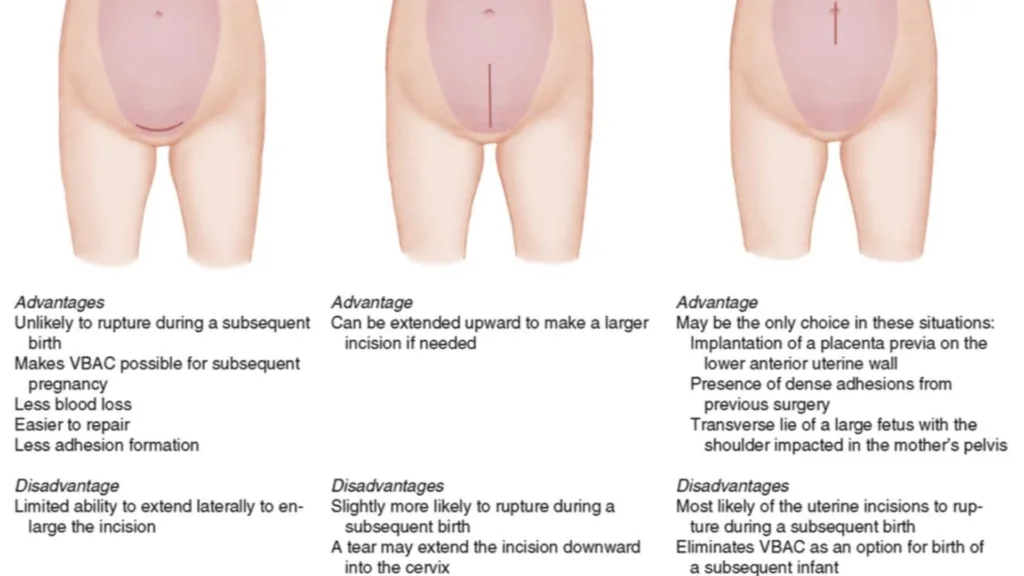
Not all women are suitable candidates. Candidates need to meet certain criteria such as having had a prior cesarean delivery with a low transverse incision and no other contraindications for vaginal birth after cesarean. Most persons are candidates if they have had one previous low transverse CD.
That means the scar on your uterus (not the skin) is horizontal in the lower part of your uterus. Such a person can be and should be counseled and offered a TOLAC if there are no other medical complications at play; candidacy is also based on individualized assessment. Even if a patient is not the best candidate, but presents to labor and delivery in active labor, clinical judgment may be used to determine the best route for delivery.
ACOG Guidelines for TOLAC
The American College of Obstetricians and Gynecologists (ACOG) provides comprehensive guidelines and recommendations regarding the trial of labor after cesarean, helping healthcare providers to make informed decisions and offer the best care to their patients.
Not A Good Candidate
- Previous classical or “T” incision
- Extensive transfundal uterine surgery (ex: with myomectomy)
- Contraindication for vaginal delivery such as placenta previa
- Prior uterine rupture-ACOG states, “…similar to a history of a prior classical cesarean, the suggested timing of delivery between 36 0/7 weeks and 37 0/7 weeks of gestation should be considered but can be individualized based on the clinical situation”.
Other Considerations:
Macrosomia (birth weight >4,000g or 4,500g)
- Less data on VBAC
- Data on uterine rupture is inconclusive
- Isolated macrosomia does ‘not preclude’ TOLAC
- Overall lower likelihood of VBAC
- It remains appropriate for obstetric care providers and patients to consider past birth weights and current estimated fetal weight when making decisions regarding TOLAC. Suspected macrosomia alone should not preclude offering TOLAC.
Gestational Age > 40 Weeks
- Decreased VBAC rates in those who attempt TOLAC
- Data on rupture conflicting
- Gestational age > 40 alone does not mean someone cannot have a TOLAC
Previous (documented) Low-Vertical incision
- Studies show a similar rate of VBAC success
- No consistent evidence of increased risk of uterine rupture or other complications
- Provider and patient may elect TOLAC
Unknown Prior Uterine Incision
- Previous case series reported VBAC success and rupture rates similar to known low transverse scars
- If one previous cesarean and unknown scar, patient may be a candidate for TOLAC if no clinical suspicion for classical incision
Twin Gestation
- Consistent evidence shows that outcomes are similar to TOLAC with singleton gestations
- Patients twin gestation and one previous low transverse scar incision are candidates for TOLAC
Obesity
- BMI alone is not an absolute contraindication to TOLAC, but should be considered an additional risk factor that may lower chance of VBAC
- Obese patients have increased risk related to CD
More than one prior CD
- Two previous low transverse CDs should be counseled and offered TOLAC
- Data limited on >2 previous CDs
Vaginal Birth After Cesarean (VBAC)
Understanding VBAC
VBAC refers to the delivery of a baby through the vagina after a previous cesarean delivery. It is a safe and appropriate option for many women who have had a prior cesarean section.
Benefits of VBAC
A successful VBAC has the following benefits:
- No abdominal surgery
- Shorter recovery period
- Lower risk of infection
- Less blood loss
Many women would like to have the experience of vaginal birth, and when successful, VBAC allows this to happen. For women planning to have more children, VBAC may help them avoid certain health problems linked to multiple cesarean deliveries. These problems can include bowel or bladder injury, hysterectomy, and problems with the placenta in future pregnancies. If you know that you want more children, this may figure into your decision.

Risks of VBAC
What are the risks of a VBAC? Some risks of a VBAC are infection, blood loss, and other complications. One rare but serious risk with VBAC is that the cesarean scar on the uterus may rupture (break open). Although a rupture of the uterus is rare, it is very serious and may harm both you and your fetus. If you are at high risk of rupture of the uterus, VBAC should not be tried.
VBAC Success Rates
In general, 50 to 60 percent of women who are considered candidates for a trial of labor after cesarean (TOLAC) to attempt vaginal birth after cesarean (VBAC) will have a successful vaginal birth (VBAC). Factors that increase the chances for a successful VBAC in an individual woman include:
- A previous vaginal delivery, especially a previous VBAC
- Spontaneous onset of labor (labor is not induced)
- Normal progress of labor, including dilation and effacement (thinning) of the cervix
- Prior cesarean delivery performed because the baby’s position was abnormal (breech)
- Only one prior cesarean delivery • The prior cesarean delivery was performed early in labor, and not after full cervical dilatation
Factors Influencing Successful VBAC
Various factors such as maternal age, birth weight, and the time interval between the previous cesarean delivery and the current pregnancy influence the likelihood of a successful VBAC.
Prediction Model for VBAC
There are prediction models available to estimate the likelihood of a successful VBAC which can aid in decision-making for both patients and healthcare providers.
Who Should Consider a TOLAC and VBAC?
- A trial of labor after cesarean (TOLAC) to attempt a vaginal birth after cesarean (VBAC) is an acceptable option for a woman who has undergone one prior cesarean delivery with a low transverse uterine incision, assuming there are no other conditions that would normally require a cesarean delivery (as an example, placenta previa)
- A woman with two prior low transverse uterine incisions or a woman who requires induction of labor may also be considered candidates for VBAC with appropriate counseling
- TOLAC with anticipated VBAC should be attempted only in those facilities capable of performing emergency cesarean deliveries





